Net Positive Initiative
A Two-Pronged Community-Empowering Approach to Improve Health
A 1st-place winning healthcare solution: an innovative and financially-viable alternative to a looming hospital system monopoly. Awarded by the University of Texas at Austin’s McComb’s School of Business’ Health Innovation Fellows and the MBA Healthcare Association.
01. Overview
OVERVIEW:
Our team, "Scheme Team" took home 1st-place grand prize of $2,500 at UT's McCombs School of Business' 3rd annual Healthcare Case Competition where a total of 8 teams competed, including participants from UC Berkeley’s Haas School of Business.
ROLES/RESPONSIBILITIES: Solution design, Illustration & Visual Development, Personas
TEAM: Daphne Hancock, MPH, Nina Lemieux, Nikhil Mahadevan, Derek Yan, Emily Yan, MS
PREPARED FOR: The University of Texas at Austin’s McCombs School of Business' 3rd annual Healthcare Case Competition
TIMEFRAME: November 2021

“Scheme Team” (Left → Right): Daphne Hancock, MPH, Nina Lemieux, Derek Yan, Emily Yan, MS, Nikhil Mahadevan

Panel of Judges: (Left → Right) Anil Swami, Lisa McDonald, MD, Andrew Well, MD/MPH, Jonathan Felix, MBA
02. Introduction
THE PROBLEM:
Teams were tasked with a real-world healthcare challenge:
In 2016, two hospital systems in a rural region of the U.S. (adjacent NE Tennessee and SW Virginia) encompassing over 1 million residents proposed a merger to create a regional hospital monopoly.
THE TASK:
Should the state of Virginia approve the hospital merger, why or why not? If so, what stipulations must be put in place to ensure the benefits to the community outweigh the possible costs of granting a monopoly? If not, what business, clinical, and operational alternative do you propose instead?
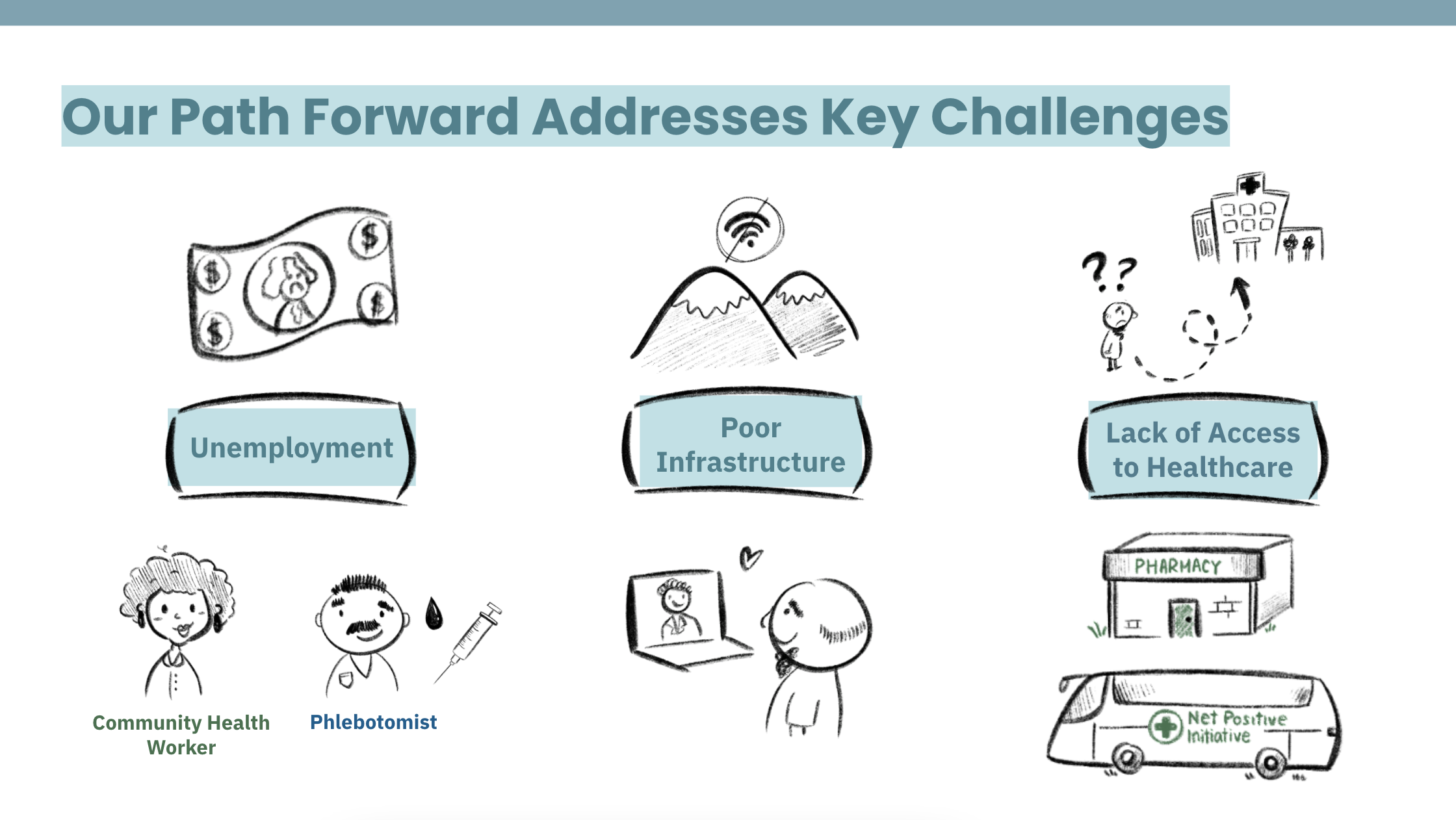
OUR HEALTHCARE SOLUTION:
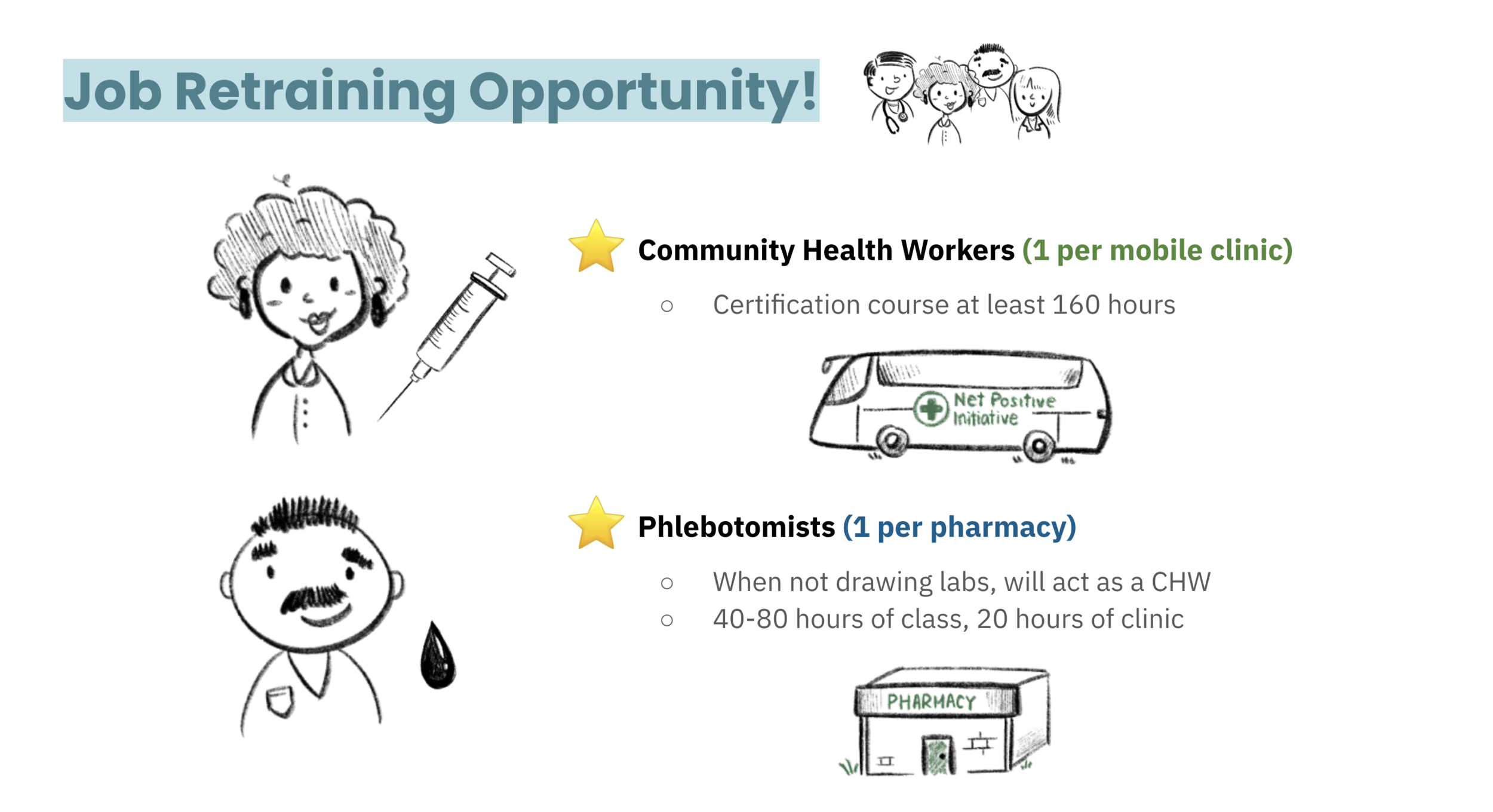
Hospital monopolies not only result in higher costs, they lead to decreased quality of care. The major healthcare challenges facing the region include unemployment, poor infrastructure, and lack of access to health care. To maintain the financial, clinical, and social health of the region, we proposed a two-pronged approach: partnerships with brick-and-mortar pharmacies in addition to mobile clinics to meet patients where they are in this rural region and employ local residents by offering them a job retraining opportunity!
03. Research
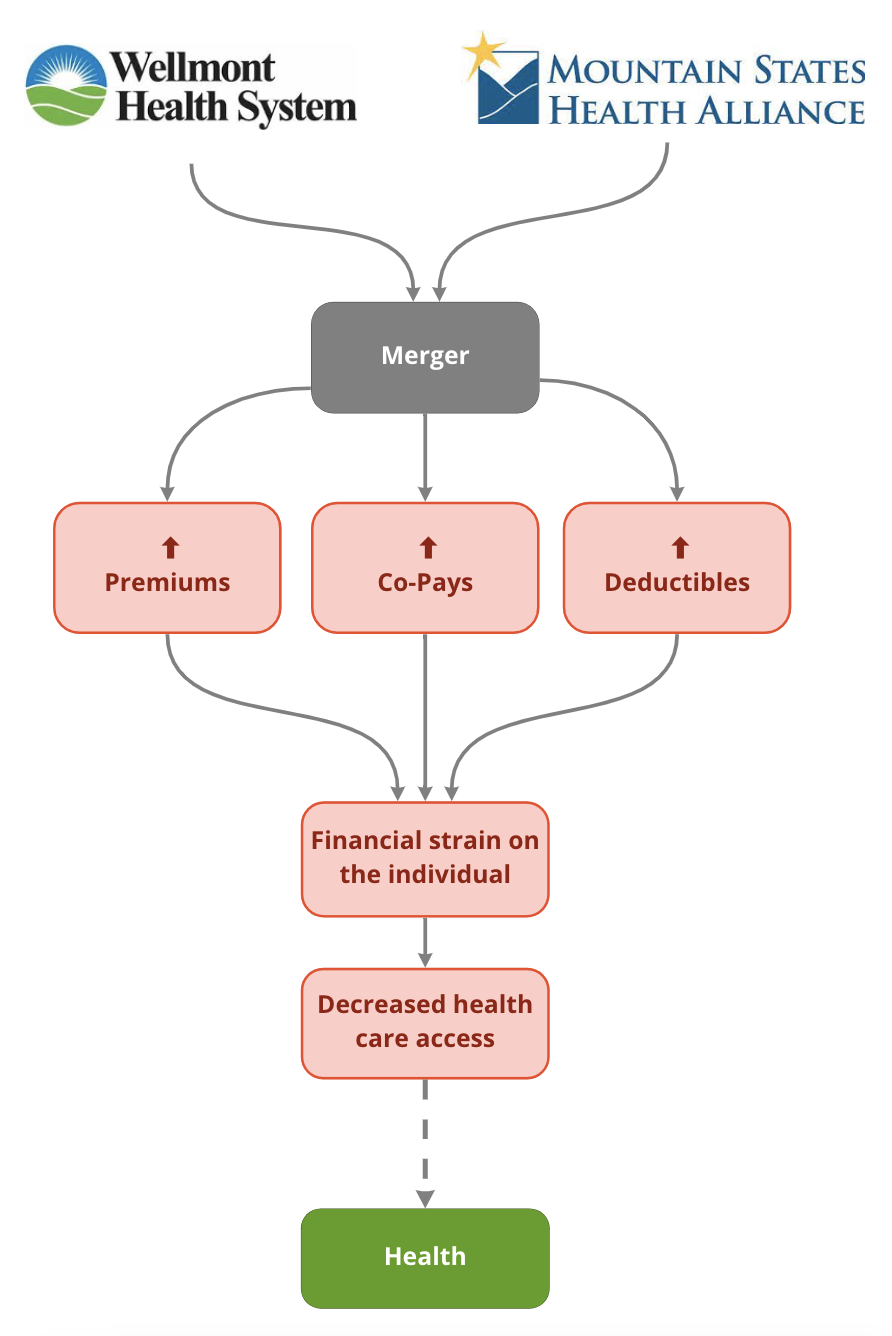
CONSEQUENCES OF A MERGER:
Our research found that hospital monopolies not only result in higher costs, they lead to decreased quality of care.
COMMUNITY FINDINGS:
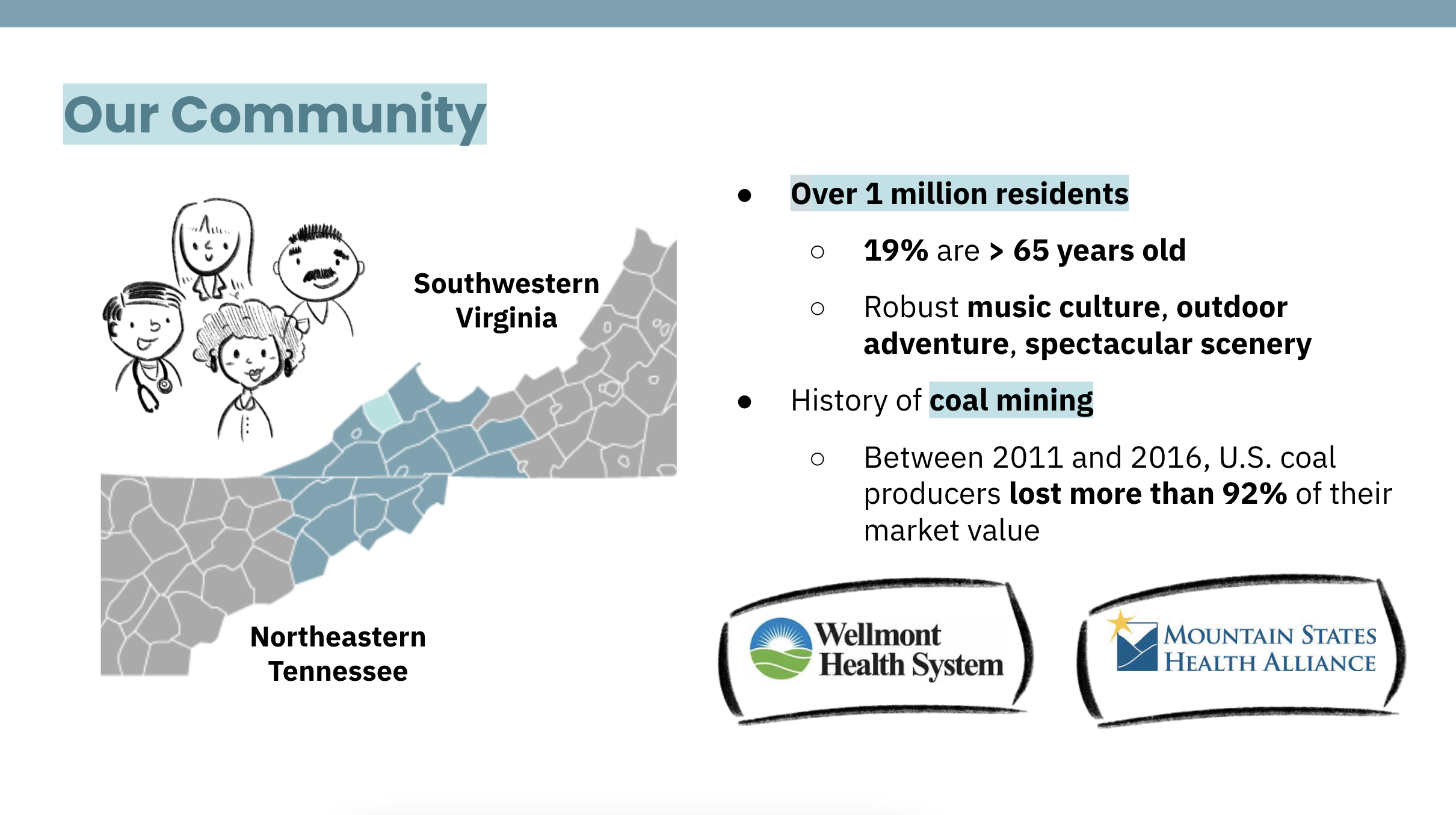
This region is home to over 1 million residents, 19% of which are > 65 years old. There is a robust music culture, outdoor adventure, and spectacular scenery.
There is also a deeply-rooted history of coal-mining. Unfortunately, between 2011 and 2016, U.S. Coal producers lost more than 92% of their market value.
Remote Access Medical (RAM) health clinics are proof-of-concept that these people will wait for and value health care. However, the crux is that these clinics pop-up just once a year.
HISTORICAL CONTEXT:
Our research found that historical hospital system mergers have failed: Mission Health in North Carolina (1995) and Benefits Health System in Montana (1996).
PROVEN ALTERNATIVES:
Formation of a monopoly is unjustified when there are alternatives:
Merge with a non-significant competitor
Health-related partnerships in rural areas have a track record of success
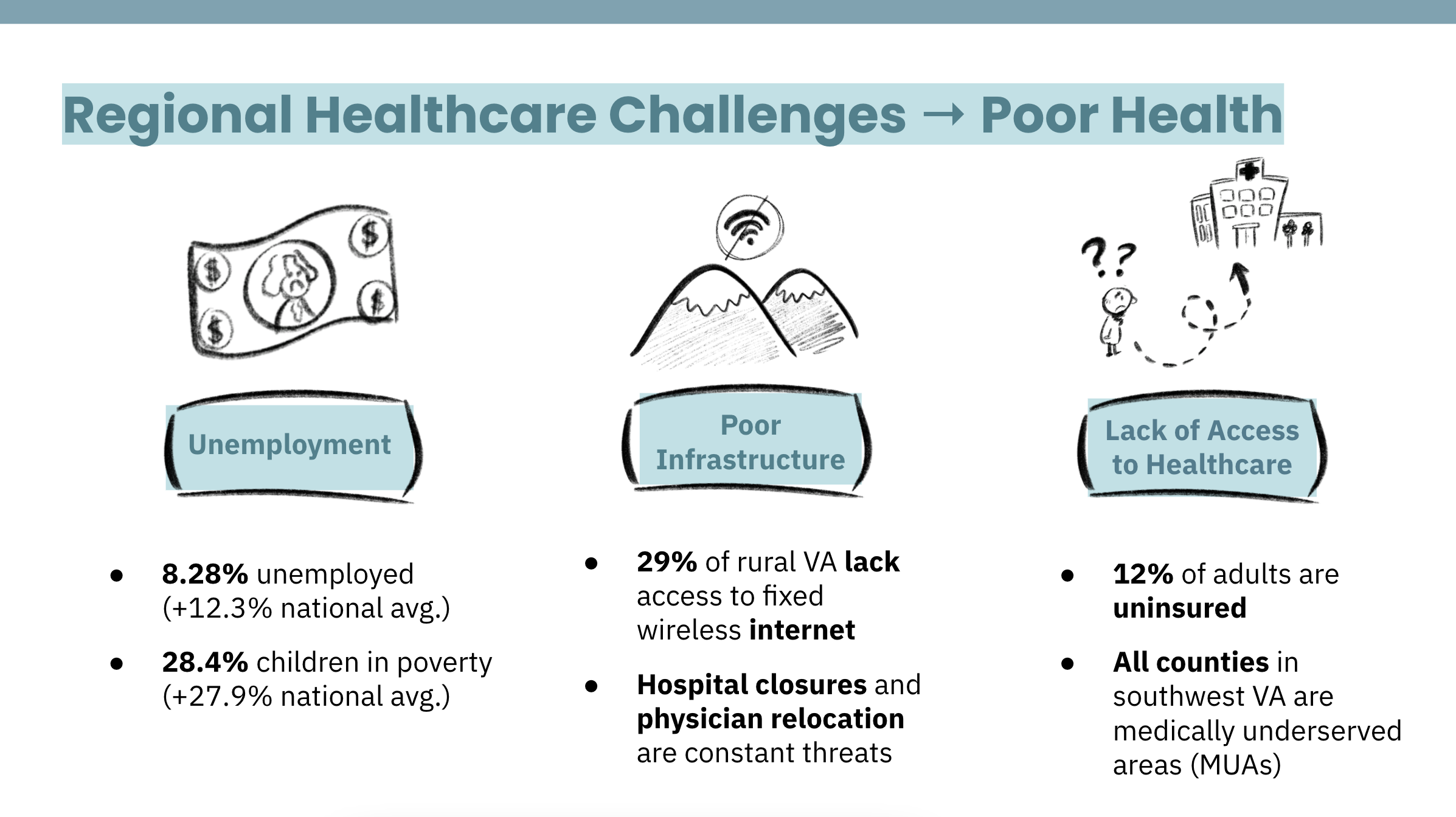
REGIONAL HEALTHCARE CHALLENGES:
Unemployment
Poor Infrastructure (Lack of Wi-fi)
Lack of Access to Healthcare
DIRECT QUOTE:
"We are proud… we don't want handouts… but we want to be able to take care of ourselves."
- Gilda Mountcastle, 54, Lee County
PERSONAS:
Dave and Denise are a few trusted, friendly faces representing newly-unemployed residents of SW Virginia's rural coal-mining towns.

INSIGHTS:
These rural community members want to be empowered to take healthcare into their own hands.
Hard-hit by unemployment, poor infrastructure, and lack of access to healthcare, this community is overdue for a solution that addresses each gap.
04. Ideation
IDEATION:
We built off of our research about mobile clinics and successful pop-up clinics in the area. Knowing the core healthcare challenges facing this region: unemployment, lack of infrastructure, and lack of access to health care, we began to ideate possible solutions in lieu of a regional hospital merger. Critical to our ideation process was knowing that folks in the area did not want handouts.

We asked ourselves:
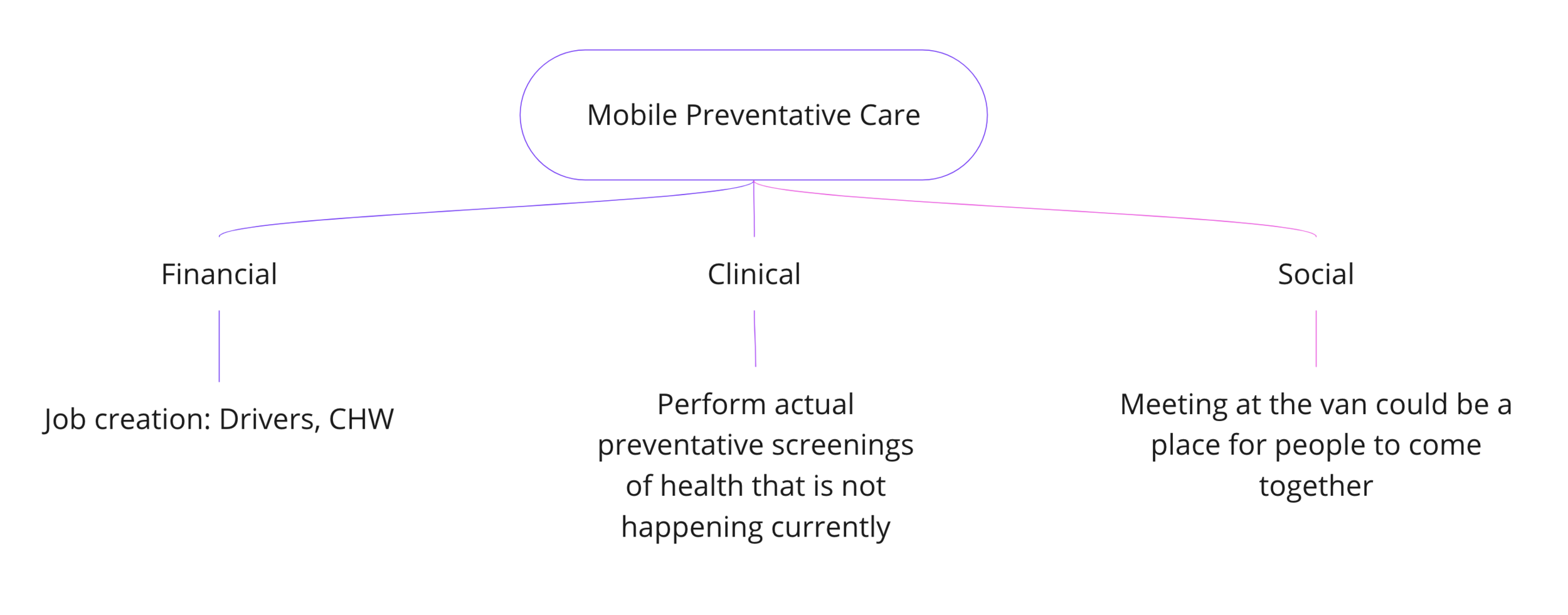
What alternative to a hospital system merger would offer the best means to improve the financial, clinical and social health of the region?
05. Prototyping
PROTOTYPING:
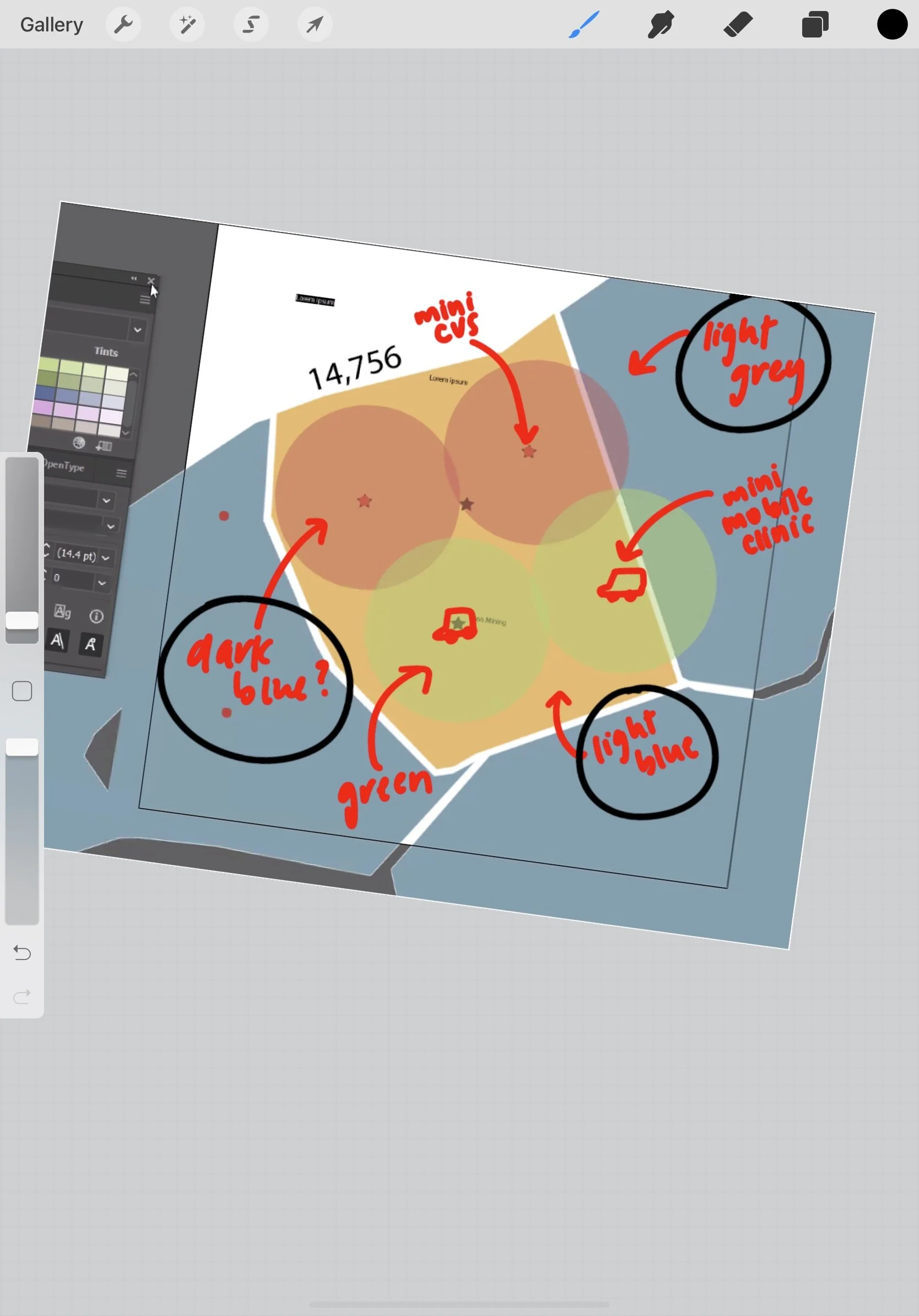
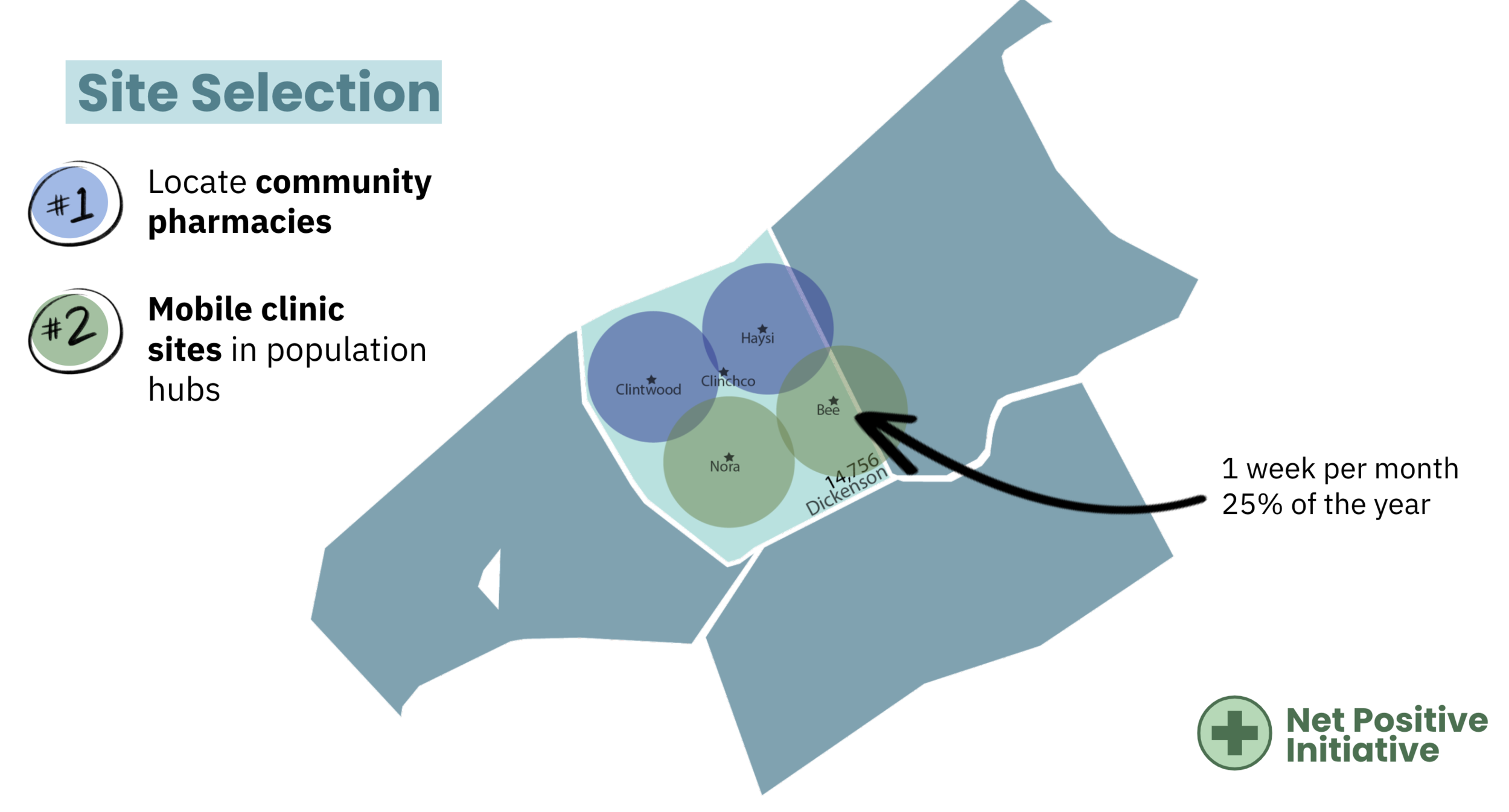
Our prototyping included mapping of where mobile clinics and pharmacy partnerships would be located in one of the most rural counties in this area. Additionally, we created a mock menu of possible health screenings that would be offered at both our brick-and-mortar pharmacy partnership locales and new wifi-enabled mobile clinics.
OUR PROPOSED ALTERNATIVE: “THE NET POSITIVE INITIATIVE”
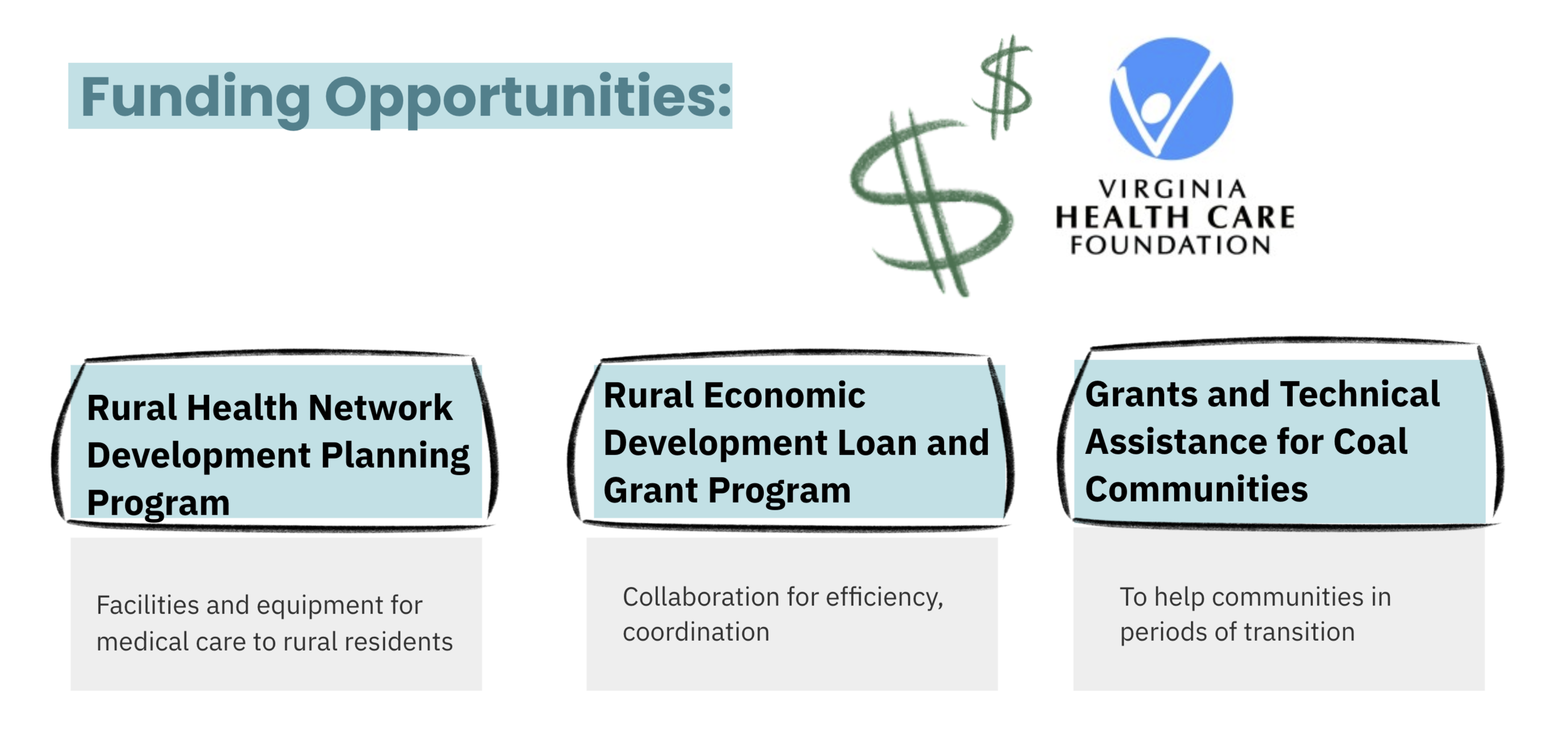
Knowing our solution needed to be financially viable, we worked together to source information about workforce availability, average wages, reimbursements for certain procedures and visits, rates of service utilization, and more to financially model our final proposal.
Ultimately, the judges praised our team for our thorough research into the region we wanted to serve and proposing a solution that empowered community members to champion preventative health in a financially sustainable way.

FUTURE COMMUNITY PARTNERSHIPS:
Edward Via College of Osteopathic Medicine (VCOM) in Virginia
YMCA
Local Community Center
FINANCIAL VIABILITY:
06. Reflection
TAKEAWAYS:
Even when limited in scope with the challenge set in 2016, I learned the value of secondary research in understanding community.
Community empowerment is invaluable.
Financial viability and feasibility must be a top priority, no matter the design challenge.

Scheme Team Members: (Left → Right) Nikhil Mahadevan, Emily Yan, MS, Nina Lemieux, Daphne Hancock MPH, Derek Yan
AWARDS & PRESS:
$2500 First-place Grand Prize
Design in Health takes 1st and 2nd place in McCombs Healthcare Case Competition
Thank you!